First Human Transplant of a Genetically Modified Pig Kidney Performed
“For the first time, surgeons have transplanted a kidney from a genetically modified pig into a living person, doctors in Boston said Thursday.
Richard Slayman, 62, of Weymouth, Mass., who is suffering from end-stage kidney disease, received the organ Saturday in a four-hour procedure, Massachusetts General Hospital announced. He is recovering well and is expected to be discharged soon, the hospital said.”
“In the nineteenth century, the invention of anesthesia was considered a gift from God. But post-operative pain relief has continued to rely on opioids, derivatives of opium, the addictive substance employed since ancient times. Although no other drug has managed to match the rapid, potent, and broadly effective relief delivered by opioids, their side effects have led to decades of addiction and overdose, leaving researchers keen to find a better solution.
This all changed in January 2025, when the FDA approved Vertex Pharmaceuticals’s Journavx (suzetrigine): the first non-opioid pain reliever suitable for treating post-surgery pain. Clinical trials found no signs of the problematic side effects associated with opioids: no drug abuse, tolerance, or withdrawal. But this was not an easy win: Vertex and other pharma companies spent decades searching for drugs like this to no avail.”
US Heart Attack Deaths Down Almost 90 Percent Since 1970
“Deaths from heart attacks have plummeted in the US over the past 50 years, whereas deaths from chronic heart conditions have skyrocketed, probably due to people living longer.
‘We’ve made some really great progress in certain areas of heart disease mortality, but now we’re seeing this shift,’ says Sara King at Stanford University in California.
She and her colleagues collected data on heart disease deaths from 1970 to 2022 using the US Centers for Disease Control and Prevention’s WONDER database, which tracks all recorded fatalities in the country.
They found that in 2022, heart disease accounted for 24 per cent of all deaths in the US, down from 41 per cent in 1970. The decline is largely thanks to an almost 90 per cent decrease in heart attack deaths, which were once the deadliest form of heart disease…
Even so, heart disease remains the country’s top killer, mainly because deaths from other types of heart disease – mostly chronic conditions – have increased 81 per cent over the same period. For instance, fatalities from heart failure, arrhythmia and hypertensive heart disease have risen 146 per cent, 106 per cent and 450 per cent, respectively.
‘A lot of these conditions are conditions that come with age,’ says King. ‘To us, it seems like people that are now surviving these heart attacks are living longer and having more time to sort of develop these chronic heart conditions.'”
Younger Generations Less Likely to Have Dementia, Study Suggests
“Writing in the journal Jama Network Open, researchers in Australia report how they analysed data from 62,437 people aged 70 and over, collected from three long-running surveys covering the US, England and parts of Europe.
The team used an algorithm that took into account participants’ responses to a host of different metrics, from the difficulties they had with everyday activities to their scores on cognitive tests, to determine whether they were likely to have dementia.
They then split the participants into eight different cohorts, representing different generations. Participants were also split into six age groups.
As expected, the researchers found the prevalence of dementia increased by age among all birth cohorts, and in each of the three regions: UK, US and Europe. However, at a given age, people in more recent generations were less likely to have dementia compared with those in earlier generations.
‘For example, in the US, among people aged 81 to 85, 25.1% of those born between 1890–1913 had dementia, compared to 15.5% of those born between 1939–1943,’ said Lenzen, adding similar trends were seen in Europe and England, although less pronounced in the latter.”
Neonatal Suffering: How We Came to Care Through Data
Evidence-based medicine gives a voice to the voiceless.
Camille Miner —
Summary: For much of modern history, newborns endured surgeries without pain relief. Doctors wrongly believed they couldn’t feel pain. This began to change in the 1980s and ’90s, when research revealed newborns’ physiological and behavioral pain responses—leading to new standards of neonatal care. The shift was driven by the rise of evidence-based medicine, which replaced tradition and expert intuition with clinical data—ultimately transforming infant surgery and global health outcomes.
Millions of newborns or “neonates” worldwide undergo invasive surgeries in their first 28 days of life. These infants are quickly put on operating tables and cut open, tubes inserted into their bodies, scalpels, and forceps probing and manipulating their organs after just entering the world. And for decades, these newborns were conscious of their pain. For the sake of successful surgeries, neonates were often given muscle relaxers to paralyze their resistance, but they still felt the sensations of scalpel incisions, open heart surgery, and chest tube insertions.
Prior to the 1980s, it was a common misconception that newborns or “neonates” did not experience severe pain. Medical experts relied on outdated theories suggesting that newborns couldn’t experience pain due to memory limitations and because their cerebral cortex had not yet undergone myelination, the process through which nerve fibers develop the capacity to rapidly transmit pain signals. General anesthesia to fully numb the neonate from pain was considered too risky for infants at the time, making experimentation unjustifiable for most researchers.
Countering this myth, in 1987, Dr. K.J.S. Anand and Dr. P.R. Hickey found that infants who undergo operations without anesthesia reported severe stress responses with steep spikes in cortisol and adrenaline levels. In their study, neonates expressed complex behavioral responses, which proved that the infants’ attempts to resist or avoid pain when not sedated were not mere reflexes. Dr. Anand later ran a randomized trial on neonates given fentanyl and found that neonates who were given no fentanyl anesthetic not only endured severe pain but suffered from “circulatory and metabolic complications postoperatively.”
Later, in 2010, scientists discovered that the nerve endings they previously thought could not communicate pain to the brain prior to myelination were signaling pain in neonates, but at a slower rate. More progress in this field is expected to continue as studies in local and regional anesthetics show that such treatments lower neonatal overdose risks and reduce opioid use.
In 1987, the American Academy of Pediatrics deemed neonatal operations without local anesthetic unethical, and US medical practices shifted to implement neonatal anesthetic. It may seem easy to assume that the medical community must not have considered them sentient beings worthy of painless procedures. However, experimenting with infants and fentanyl is not without its risks. Thus, doctors had reason to perpetuate tradition and old expert practices of anesthetic-free procedures, even if at the cost of infant suffering.
The true impetus for change in neonatal treatment was not mere compassion but a transformative paradigm shift in medical practice. While clinical research was not new to medicine, previously, doctors often favored expert opinion by the doctors with respected practice and reputation. However, doctors like Dr. Gordon Guyatt of McMaster University made a formal push in the 1990s for “Evidence-Based Medicine” (EBM), which “de-emphasizes intuition, unsystematic clinical experience, and pathophysiologic rationale as sufficient grounds for clinical decision making and stresses the examination of evidence from clinical research.” Put another way, the opinions of individual doctors would not take precedence over evidence-backed medical research.
The previous reliance on expert opinion created biased data and a lack of standardization for procedural techniques and diagnoses. Thus, a doctor in California could perform hernia repair surgery in a technique radically different from a doctor in New York. But, as the EBM movement advocated, it is unlikely that two differing procedures have identical success rates. After realizing the benefits of prioritizing systematic reviews/meta-analyses, cross-sectional studies, and randomized control trials over the experiences of seasoned doctors, the medical community was capable of greater safe experimentation and findings. Additionally, with the onset of digitized medical records, tracking medical data over time is much faster and cheaper. Thanks to the efforts of clinical researchers and evidence favoring doctors, we live in a world filled with data and research capable of tailoring high-risk anesthetics to the infants who just entered our world.
Over the past four decades, the use of anesthesia for newborns has become more standardized in all developed countries. Furthermore, with the globalization of medical knowledge, more low and middle-income countries have access to advanced anesthetic treatments capable of safely sedating infants and preventing severe pain in operations. Digitization of medical records, remote training, and the standardization of best practices have together increased global access to neonatal anesthesia.
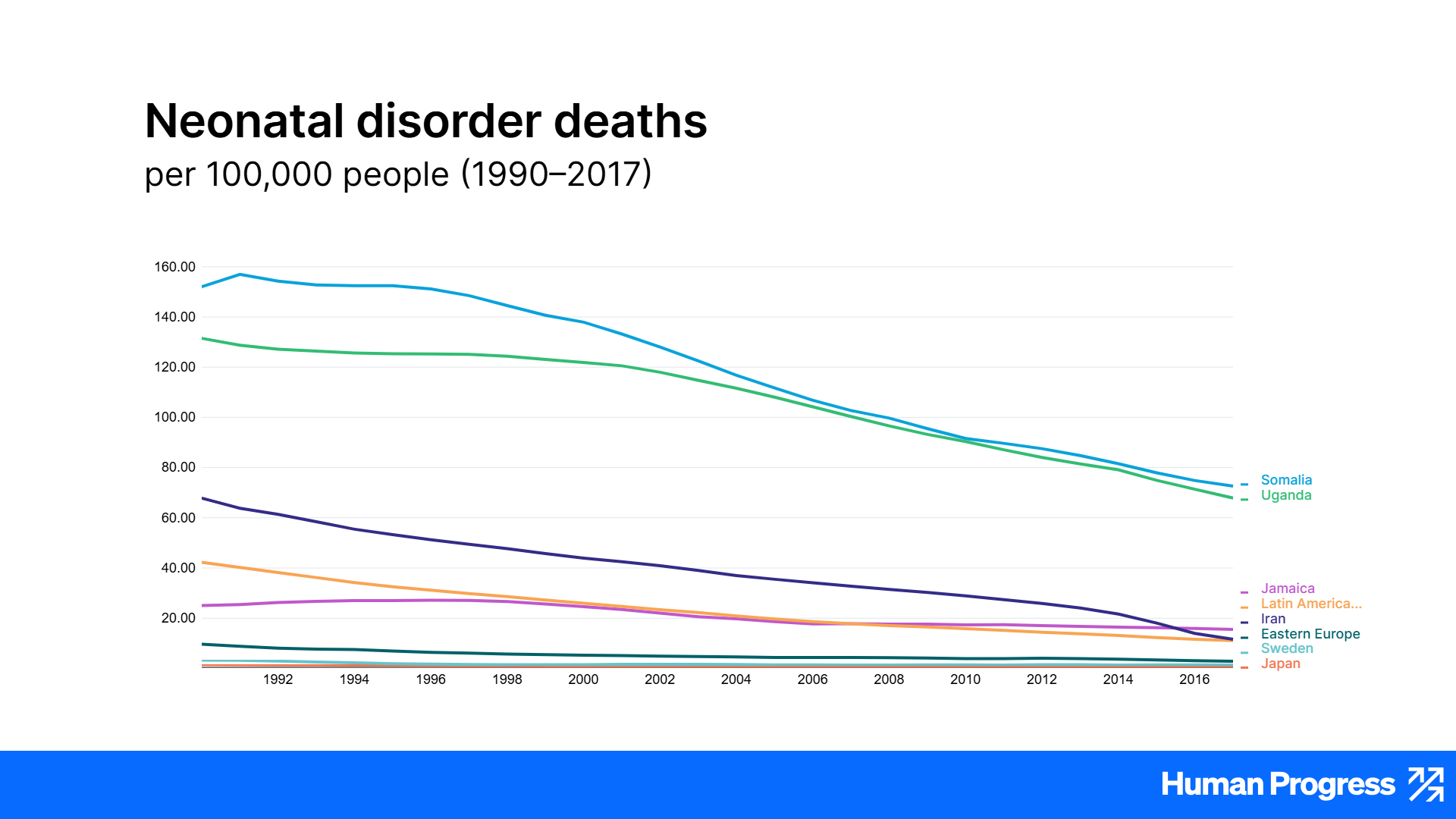
Furthermore, according to the Institute For Health Metrics and Evaluation, newborn deaths preventable by neonatal surgery (e.g., congenital defects and birth trauma injuries) have also been on a steep decline since the international standardization of medicine and the onset of global health initiatives. On the whole, neonatal disorder deaths are steeply declining. That’s partly a consequence of surgery—now with safe neonatal anesthetic. With more advanced medical practices and anesthetic procedures now shared with and adopted by developing countries, global inequality in infant welfare overall is decreasing.
This transformation in neonatal concern not only represents our increased sensitivity to human suffering but also demonstrates how valuing empirical research enables us to identify and prevent such harm.